Int J Drug Res Clin. 2023;1:e3.
doi: 10.34172/ijdrc.2023.e3
Original Article
Pain Management in Trauma Patients Referred to the Emergency Department of Imam Reza General Hospital, Tabriz, Iran
Amir Ghaffarzad 1  , Farzad Rahmani 1, Zahra Parsian 2 , Minoo Arefikia 3, Fariba Abdollahi 4, Hamid Reza Morteza Bagi 1, *
, Farzad Rahmani 1, Zahra Parsian 2 , Minoo Arefikia 3, Fariba Abdollahi 4, Hamid Reza Morteza Bagi 1, *
Author information:
1Emergency and Trauma Care Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
2Clinical Fellow Leeds Teaching Hospitals NHS TRUST, England, United Kingdom
3Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
4Clinical Skills Center, Faculty of Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Background:
Trauma patients with acute pain are often triaged when experiencing less pain than urgency level; therefore, they have to wait longer to receive analgesics.
Methods:
The data was collected using Numerical Rating Scale (NRS) and a checklist. After data collection, descriptive statistical methods (tables, graphs, and mean±standard deviation) and analytical statistics (ANOVA, Kruskal-Wallis, and chi-square tests) were used to analyze the data in SPSS version 20.0.
Results:
The pain intensity score (mean±standard deviation) of patients at admission and discharge from the medical center was 7.81±0.89 and 3.69±0.49, respectively. The mean time of the patient’s first visit was 3.47±15.20 minutes. According to Kruskal-Wallis nonparametric test, there was a statistically significant difference in the duration of patients’ examination by a physician (P<0.001). The waiting time for the first treatment to relieve the pain was 13.5±3.6 minutes. In patients referred to the emergency department, the satisfaction rate was 97.4%.
Conclusion:
Narcotics were the most commonly used analgesic drug with immediate effect on pain reduction. The patients’ satisfaction with pain relief was ideal.
Keywords: Trauma patients, Emergency department, Pain management, Analgesia
Introduction
Pain complaints are common in trauma patients.1 Pain in trauma patients is a double-edged sword. On the one hand, it is a good indicator for estimating the severity and type of injury. On the other hand, lack of pain reduction causes severe complications.2 Trauma patients with acute pain, especially with musculoskeletal injury, are often triaged when their pain severity is less than the urgency level, and their pain relief takes more time. Studies have shown that in 95% of trauma patients whose pain intensity was estimated by the nurse, pain control was inadequate.3 Pain management in trauma patients referred to the emergency department is often done using non-pharmacological techniques such as splinting or prescribing several different drugs, especially non-steroidal anti-inflammatory drugs.4 Although proper pain management in trauma patients is not enough, studies have shown that proper pain control reduces morbidity and improves treatment outcomes. Although pain management is one of the main factors in the emergency ward, it is still inappropriate and inadequate.5 A study conducted in the United States and Canada found that 60% of patients receive analgesics long after the admission, and 74% of patients are discharged from the emergency ward when their pain level is between moderate to severe.6
Lack of proper pain control may cause physiological complications such as unstable hemodynamic status, sleep disturbance, and immune system disorders, as well as psychological complications such as anxiety, post-traumatic stress disorder, and impaired consciousness. Therefore, pain management is not only an essential factor in the emergency department but also is ethically, legally, and clinically an important issue.3 Despite many pain management intervention strategies, studies have shown that pain control is not appropriate in the emergency department. Inaccurate estimation of the pain level, excessive pain relief, and administration of inappropriate analgesics are common in the emergency department.7,8
Therefore, in this study, the researcher has studied pain management in trauma patients referred to the emergency department of Imam Reza General Hospital in Tabriz in 2019. The results of the study can be used to enhance the quality of medical services to protect patients’ rights.
Methods
In this descriptive-analytical cross-sectional study, all patients who met inclusion criteria and referred to the emergency department of Imam Reza General Hospital of Tabriz University of Medical Sciences (referral center for trauma patients in the northwest of the country) in the first 3 months of 2019 were included in the study by census method. The sample size included 385 patients according to the admission rate of trauma patients in one year (40 000 people), using Morgan table and with the probability of excluded samples. Trauma patients over 18 years of age with stable hemodynamic status, Glasgow Coma Scale (GCS) over 13, and the ability to answer questions and feel pain were included in the study. Exclusion criteria included lack of interest in participating in the study, unstable hemodynamic status in less than 4 hours of admission, and transfer to another ward.
The researcher collected data by explaining the method and purpose of the study and obtaining informed consent from the patients or their next of kin. The data were collected orally using Numerical Rating Scale (NRS) and a researcher-made checklist. The checklist is a set of items about the patient demographics (age, sex, etc.) and disease information (trauma mechanism, location of pain, cause of trauma, etc). Finally, the data were analyzed using descriptive statistical methods (tables, graphs, and mean ± standard deviation) and analytical statistics (ANOVA, Kruskal-Wallis, and Mann-Whitney tests) in SPSS version 20.0.
Results
According to the patient demographics, 298 of all participants (77.4%) were male and 87 (22.6%) were female. The mean age of the participants was 17.78 ± 35.41 years. The majority of injuries to the lower limbs (40.3%) and head and neck (37.9%) were due to traffic accidents (91.2%).
Pain Intensity in Trauma Patients
The mean pain intensity score of the patients participating in this study at admission, half an hour, one hour, two hours, three hours, and four hours after admission was equal to 7.81 ± 0.89, 3.56 ± 1.27, 3.39 ± 0.65, 3.0 ± 63.65, 3.0 ± 78.65, and 3.71 ± 0.54. Based on the results of repeated measures ANOVA (Figure 1), changes in pain intensity of trauma patients during treatment were statistically significant (P < 0.001).
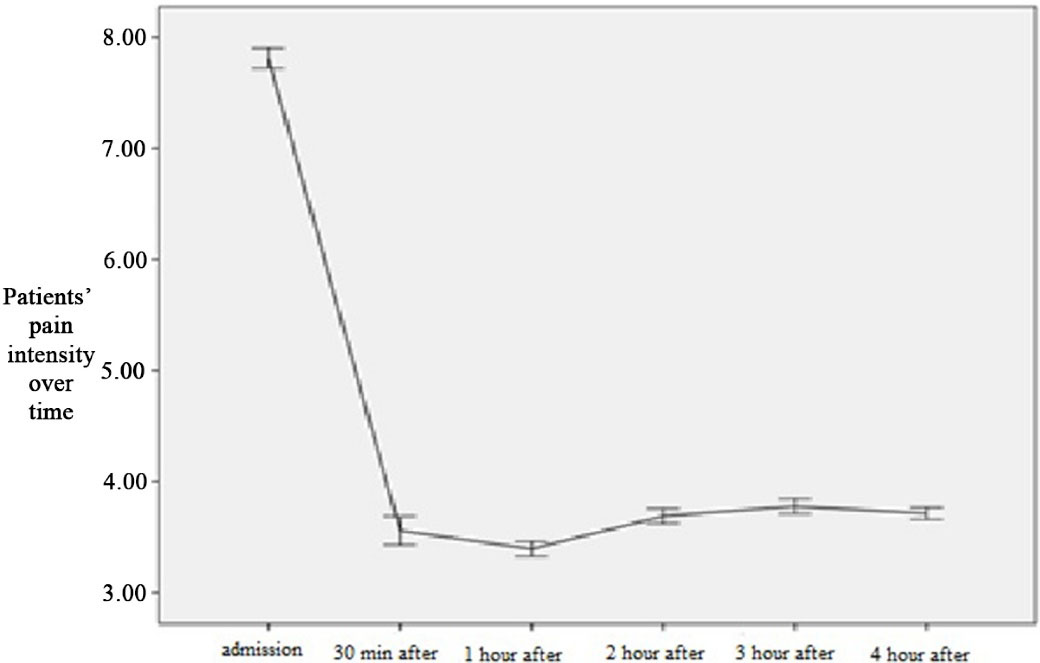
Figure 1.
Patients’ Pain Intensity over Time
.
Patients’ Pain Intensity over Time
Pain Intensity in Trauma Patients Based on the Type of Treatment
Table 1 and Figure 2 show the mean pain intensity of patients over time based on the type of treatment. Based on the results of repeated measures ANOVA, type and time of treatment had a significant effect on patients’ pain intensity (P < 0.001).
Table 1.
The Mean Pain Intensity Score of Patients Over Time Based on the Type of Treatment
|
Time
|
Type of Treatment
|
Mean
|
SD
|
P
value (Type of Treatment)
|
P
Value (Time)
|
| Pain intensity at admission |
Morphine |
7.97 |
0.76 |
< 0.001 |
< 0.001 |
| Ketamine |
8.06 |
1.01 |
| Pethidine |
7.71 |
0.64 |
| Apotel |
7.14 |
1.39 |
| Pain intensity 30 minutes after admission |
Morphine |
3.66 |
1.15 |
| Ketamine |
3.85 |
1.64 |
| Pethidine |
2.80 |
0.76 |
| Apotel |
4.70 |
1.21 |
| Pain intensity 1 hour after admission |
Morphine |
3.50 |
0.68 |
| Ketamine |
3.38 |
0.64 |
| Pethidine |
3.20 |
0.56 |
| Apotel |
3.43 |
0.66 |
| Pain intensity 2 hours after admission |
Morphine |
3.81 |
0.70 |
| Ketamine |
3.57 |
0.68 |
| Pethidine |
3.50 |
0.50 |
| Apotel |
3.75 |
0.65 |
| Pain intensity 3 hours after admission |
Morphine |
3.86 |
0.72 |
| Ketamine |
3.70 |
0.83 |
| Pethidine |
3.72 |
0.45 |
| Apotel |
3.64 |
0.49 |
| Pain intensity 4 hours after admission |
Morphine |
3.72 |
0.59 |
| Ketamine |
3.51 |
0.62 |
| Pethidine |
3.80 |
0.40 |
| Apotel |
3.68 |
0.47 |
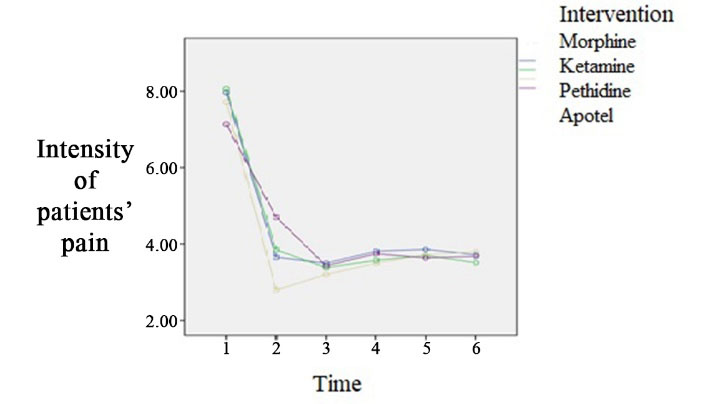
Figure 2.
The Pain Intensity of the Patients over Time Based on the Type of Treatment
.
The Pain Intensity of the Patients over Time Based on the Type of Treatment
Pain Intensity in Trauma Patients Based on the Type of Injury
Based on the results of repeated measures ANOVA, injury type and time had a significant effect on patients’ pain intensity (P < 0.05). Figure 3 shows the mean pain intensity of patients over time based on the type of injury.
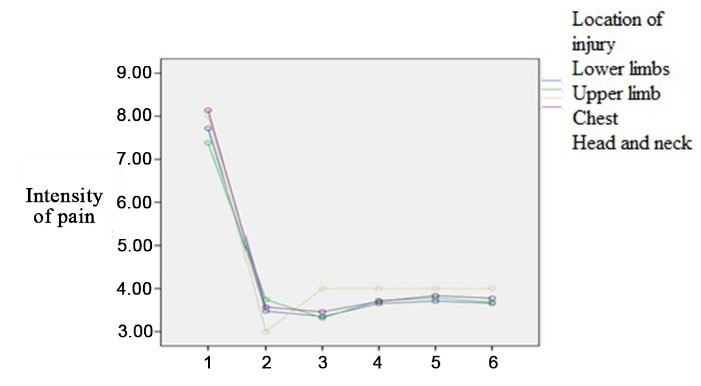
Figure 3.
The Pain Intensity of the Patients over Time Based on the Location of the Injury
.
The Pain Intensity of the Patients over Time Based on the Location of the Injury
Intensity of Pain during Discharge
The mean pain intensity score of the patients at admission and discharge from the medical center was 7.81 ± 0.89 and 3.69 ± 0.49, respectively. Based on the results of paired t-test, this difference was statistically significant. Table 2 shows the intensity of patients’ pain at discharge based on the type of treatment. According to one-way ANOVA, there was not any statistically significant difference in the mean pain intensity at the time of patients’ discharge.
Table 2.
The Mean Pain Intensity Score of Patients at the Time of Discharge Based on the Type of Treatment
|
Type of Treatmnet
|
Number of Patients
|
Mean
|
SD
|
P
Value
|
| Morphine |
186 |
3.67 |
0.53 |
0.05 |
| Ketamine |
47 |
3.57 |
0.54 |
| Pethidine |
108 |
3.80 |
0.40 |
| Apotel |
44 |
3.68 |
0.47 |
Duration of the First Examination of the Patient by a Physician or Nurse
The mean time of the first visit by a physician in trauma patients referred to the emergency department was 3.47 ± 15.20 minutes. This time was 18.33 ± 2.58 minutes for patients with chest injuries and 13.53 ± 2.64 minutes for patients with head and neck injuries, respectively. According to Kruskal-Wallis test, there was a statistically significant difference in the duration of patients’ examination by a physician (P < 0.001).
Waiting Time for Pain Relief Treatment
On average, trauma patients referred to the treatment center waited 13.5 ± 3.6 minutes to receive the first clinical treatment for pain relief. According to Kruskal-Wallis test, the waiting time to receive clinical intervention to reduce pain in trauma patients based on the type of injury was not statistically significant (P = 0.31), indicating that this duration was lowest in patients with upper limb injuries and highest in patients with chest injuries.
Type of Clinical Treatments to Reduce Pain in Trauma Patients
In the patients participated in this study, the highest doses of morphine, ketamine, pethidine, and Apotel were injected into patients with lower limb, head and neck, lower limb, and head and neck injuries, respectively. Based on chi-square test, there was a statistically significant difference in the type of injury and type of treatment. Table 3 shows the number and percentage of clinical treatments based on the type of injury.
Table 3.
Number and Percentage of Treatment Measures by Type of Injury
|
Type of Treatment
|
Location of Injury
|
P
Value
|
|
Lower Limbs
|
Upper Limb
|
Chest
|
Head and Neck
|
| Morphine |
Number |
92 |
28 |
2 |
64 |
0.004 |
| Percent |
49.5 |
15.1 |
1.1 |
34.4 |
| Ketamine |
Number |
14 |
14 |
0 |
19 |
| Percent |
29.8 |
29.8 |
0.0 |
40.4 |
| Pethidine |
Number |
32 |
22 |
4 |
50 |
| Percent |
29.6 |
20.4 |
3.7 |
46.3 |
| Apotel |
Number |
17 |
14 |
0 |
13 |
| Percent |
38.6 |
31.8 |
0.0 |
29.5 |
Frequency of Assessment of Pain Reduction in Trauma Patients
All patients participating in this study were evaluated 6 times to assess pain relief after performing a clinical treatment by a physician or nurse.
Satisfaction of Trauma Patients with Pain Control in the Emergency Department
The satisfaction rate of patients referred to the emergency department of Imam Reza Medical Center was 97.4%. Out of the total number of patients, 10 were dissatisfied with the treatment, of whom 5 had lower limb injuries and 5 had upper limb injuries.
Discussion
Proper pain management in trauma patients requires proper assessment of the pain intensity, identification of an appropriate analgesic drug based on the patient’s pain intensity, accurate knowledge of the side effects of analgesic drugs, and frequent evaluation of the patient’s pain.9 This study showed that the majority of patients had severe pain at the time of admission (7.81 ± 0.89) and the patients’ pain was statistically reduced over time (3.55 ± 1.27), which was not clinically sufficient because patients reported moderate pain at the time of discharge from the emergency department or transfer to another ward. Pierik et al reported that patients with musculoskeletal trauma reported severe pain at the time of admission (6.5) and discharge (5.6), indicating poor pain control in these patients.3
Although pain management in trauma patients is not sufficient, studies have shown that proper pain control reduces morbidity and improves treatment outcomes.5 Despite the extensive knowledge of pain management as one of the main factors in treatment in the emergency department, research shows that pain management in the emergency department is still inappropriate and inadequate.5 A study in the United States and Canada found that 60% of patients receive analgesics long after the admission, and 74% of patients are discharged from the emergency room while experiencing moderate to severe pain.6
Masoudi Alavi et al reported inadequate pain management in trauma patients,9 and in a study conducted in New Zealand, 98.9% and 97.7% of patients with musculoskeletal trauma reported high-intensity pain at admission and discharge, respectively.3
In this study, the injection of ketamine, morphine, pethidine, and Aptol was administered for the maximum to minimum pain intensity at the time of admission, respectively, and the type of medical treatment used had no effect on reducing pain at discharge. In the patients participated in this study, the highest doses of morphine, ketamine, pethidine, and Apotel were injected into patients with lower limb and head and neck injuries, respectively. According to guidelines on pain control, the type of medication depends on the degree of injury to patients. In patients with severe pain, opioids are used frequently.10 The four most common drugs used to control pain in the emergency department are morphine, meperidine, fentanyl, and hydromorphone.11
Morphine is one of the main opioids in pain relief in emergency patients due to its easy availability.12
Rapid administration of low-dose intravenous narcotics at frequent intervals to relieve pain has been recommended in most studies to provide an opportunity for the physician to manage the patient’s basic needs.4
The results of a multicenter study from 22 countries showed that in 92.5% and 67.5% of cases, morphine and paracetamol were respectively the most commonly used painkillers in the emergency department to control severe pain in patients.13 These results are in line with the present study in that morphine is the most widely used drug.
In a study by Grenman et al in Finland, severe pain was reported by 45.8% of patients and 46.4% of patients in the emergency department received analgesic medication,7 which is in line with our study that analgesia was given to all patients with high pain intensity.
In another study, 36% of patients in the United States,14 74.9% of patients in Australia,15 42% of patients in Canada,6 and 46% of patients in Iran in the emergency department did not receive painkillers despite severe pain.9 However, during pain control, the best way to reduce pain in the emergency room is to prescribe painkillers.9
In this study, the mean waiting time for the first examination of a patient’s pain by a physician or nurse was 15.20 minutes. The results show that because patients with head and neck injuries reported the highest pain intensity, the first pain assessment of these patients was performed in the shortest time of 13.53 minutes, although the maximum waiting time for pain assessment was 18.33 minutes for patients with injuries to the chest. Moreover, the waiting time for receiving the first treatment to reduce pain (3.6) was 13.5 minutes. This time was the lowest for patients with upper limb injuries and the highest for patients with chest injuries.
Despite the severe pain of most emergency patients, studies show that patients have to endure severe pain for a long time before receiving painkillers.14 The mean waiting time for the patient’s first assessment of pain since the admission was 41 minutes in a study by Masoudi Alavi et al,9 100 minutes in a study by Minick et al14, and 41 minutes after admission in a study conducted in Canada.6
The pain control protocol in the emergency department states that patients with severe pain should receive analgesics within 30 minutes of triage.16 Fortunately, in this study, patients did not wait long to receive painkillers, indicating that emergency personnel managed the patient’s pain.
Frequency of Assessment of Pain Relief in Trauma Patients
All patients participating in this study were evaluated 6 times to check pain relief after a clinical treatment by a physician or nurse. Improper pain management leads to prolonged hospitalization, readmission, and dissatisfaction with medical care17,18 and ultimately leads to unwellness and a high rate of patient mortality.18,19 For proper management and control of pain, several assessments of pain and individual treatment based on the patient’s condition are needed.20 Besides, re-examination of pain allows the evaluation of the effect of pharmacological and non-pharmacological interventions. Bucknall et al reexamined pain in only 4.4 cases.3
The effectiveness of treatment cannot be adjusted according to the patient’s needs if there is no report of pain management, which is not appropriate due to the lack of traceability of treatment and ongoing treatment. Winslow and Kaiser as well as Wells et al suggested that measuring pain as the fifth vital sign and using pain assessment tools may be effective in improving the performance of nurses in recording and controlling patients’ pain.21
Satisfaction of Trauma Patients with Pain Control in the Emergency Department
In this study, patient’s satisfaction with pain control in the emergency department was 97.4%. The results of studies show that effective and appropriate pain management can affect patient’s satisfaction with the quality of care provided.22
According to a study in the United States, pain relief is associated with increased patient satisfaction.22 Therefore, pain management should be considered an important factor in healthcare services. Overcrowding in emergency departments, lack of access to narcotics, insufficient knowledge of prescribing painkillers, and insufficient emergency resources are some of the factors that can affect pain management.8,15
Pain is one of the most unpleasant experiences of patients admitted to medical centers. In addition to the pain that the patient suffers from the existing disease, there are cases of pain due to therapeutic and diagnostic interventions in hospital wards, especially in the emergency department for hospitalized patients. Since the mentioned interventions are necessary in the process of treating patients, prevention and control of pain caused by these interventions are very important.18
Based on the results of this study and the findings of similar studies, gender and age have no effect on the pain management process.23
Conclusion
Based on the present results, pain control by analgesic medication in the emergency department of Imam Reza General Hospital in all patients was performed in the first 20 minutes of admission and the pain intensity of patients at discharge or transfer to another ward was between mild to moderate. The most commonly used analgesic drug was narcotic analgesics, which immediately reduced pain. In this study, patient’s satisfaction with pain relief was ideal.
Ethics statement
The Ethics Committee of Tabriz University of Medical Sciences has approved the present study (IR.TBZMED.REC.1397.713). All aspects of the present study were explained to patients and written informed consent was obtained from the participants or their next of kin.
Disclosure of funding source
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interests declaration
The authors report no conflict of interests.
Acknowledgments
The authors would like to appreciate the cooperation of the Clinical Research Development Unit, Imam Reza General Hospital, Tabriz, Iran, in conducting this research. This article was written based on a dataset of Minoo Arefikia’s Medical Specialty degree thesis entitled, “Pain Management in Trauma Patients Referred to the Emergency Department of Imam Reza General Hospital, Tabriz, Iran.” This study was registered at Tabriz University of Medical Sciences (Code No: 60284).
References
- Thomas V, Heath M, Rose D, Flory P. Psychological characteristics and the effectiveness of patient-controlled analgesia. Br J Anaesth 1995; 74(3):271-6. doi: 10.1093/bja/74.3.271 [Crossref] [ Google Scholar]
- Ahmadi A, Bazargan-Hejazi S, Heidari Zadie Z, Euasobhon P, Ketumarn P, Karbasfrushan A. Pain management in trauma: a review study. J Inj Violence Res 2016; 8(2):89-98. doi: 10.5249/jivr.v8i2.707 [Crossref] [ Google Scholar]
- Pierik JG, IJzerman MJ, Gaakeer MI, Berben SA, van Eenennaam FL, van Vugt AB. Pain management in the emergency chain: the use and effectiveness of pain management in patients with acute musculoskeletal pain. Pain Med 2015; 16(5):970-84. doi: 10.1111/pme.12668 [Crossref] [ Google Scholar]
- Pak SC, Micalos PS, Maria SJ, Lord B. Nonpharmacological interventions for pain management in paramedicine and the emergency setting: a review of the literature. Evid Based Complement Alternat Med 2015; 2015:873039. doi: 10.1155/2015/873039 [Crossref] [ Google Scholar]
- Nesek Adam V, Mršić V, Matolić M, Tonković D, Rašić Ž, Matejić T. Stress and pain in emergency and trauma patients. Period Biol 2013; 115(2):135-8. [ Google Scholar]
- Todd KH, Ducharme J, Choiniere M, Crandall CS, Fosnocht DE, Homel P. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain 2007; 8(6):460-6. doi: 10.1016/j.jpain.2006.12.005 [Crossref] [ Google Scholar]
- Grenman D, Niemi-Murola L, Kalso E. Management of pain in a surgical emergency unit—underlying factors affecting its delivery. Acute Pain 2008; 10(3-4):137-44. doi: 10.1016/j.acpain.2008.05.013 [Crossref] [ Google Scholar]
- Rampanjato RM, Florence M, Patrick NC, Finucane BT. Factors influencing pain management by nurses in emergency departments in Central Africa. Emerg Med J 2007; 24(7):475-6. doi: 10.1136/emj.2006.045815 [Crossref] [ Google Scholar]
- Masoudi Alavi N, Aboutalebi MS, Sadat Z. Pain management of trauma patients in the emergency department: a study in a public hospital in Iran. Int Emerg Nurs 2017; 33:53-8. doi: 10.1016/j.ienj.2016.10.005 [Crossref] [ Google Scholar]
- Yeager MP, Glass DD, Neff RK, Brinck-Johnsen T. Epidural anesthesia and analgesia in high-risk surgical patients. Anesthesiology 1987; 66(6):729-36. doi: 10.1097/00000542-198706000-00004 [Crossref] [ Google Scholar]
- Rosenow EC 3rd, Myers JL, Swensen SJ, Pisani RJ. Drug-induced pulmonary disease An update. Chest 1992; 102(1):239-50. doi: 10.1378/chest.102.1.239 [Crossref] [ Google Scholar]
- Whipple JK, Lewis KS, Quebbeman EJ, Wolff M, Gottlieb MS, Medicus-Bringa M. Analysis of pain management in critically ill patients. Pharmacotherapy 1995; 15(5):592-9. doi: 10.1002/j.1875-9114.1995.tb02868.x [Crossref] [ Google Scholar]
- Parnass AJ, Greenbaum NR, Glick MA, Halpern P. Pain management framework in the emergency department: patterns in 40 emergency departments worldwide. Eur J Emerg Med 2016; 23(4):311-4. doi: 10.1097/mej.0000000000000299 [Crossref] [ Google Scholar]
- Minick P, Clark PC, Dalton JA, Horne E, Greene D, Brown M. Long-bone fracture pain management in the emergency department. J Emerg Nurs 2012; 38(3):211-7. doi: 10.1016/j.jen.2010.11.001 [Crossref] [ Google Scholar]
- Fry M, Bennetts S, Huckson S. An Australian audit of ED pain management patterns. J Emerg Nurs 2011; 37(3):269-74. doi: 10.1016/j.jen.2010.03.007 [Crossref] [ Google Scholar]
- Patrick PA, Rosenthal BM, Iezzi CA, Brand DA. Timely pain management in the emergency department. J Emerg Med 2015; 48(3):267-73. doi: 10.1016/j.jemermed.2014.09.009 [Crossref] [ Google Scholar]
- Payen JF, Bosson JL, Chanques G, Mantz J, Labarere J. Pain assessment is associated with decreased duration of mechanical ventilation in the intensive care unit: a post Hoc analysis of the DOLOREA study. Anesthesiology 2009; 111(6):1308-16. doi: 10.1097/ALN.0b013e3181c0d4f0 [Crossref] [ Google Scholar]
- Arbour C, Gélinas C, Michaud C. Impact of the implementation of the critical-care pain observation tool (CPOT) on pain management and clinical outcomes in mechanically ventilated trauma intensive care unit patients: a pilot study. J Trauma Nurs 2011; 18(1):52-60. [ Google Scholar]
- Shannon K, Bucknall T. Pain assessment in critical care: what have we learnt from research. Intensive Crit Care Nurs 2003; 19(3):154-62. doi: 10.1016/s0964-3397(03)00027-2 [Crossref] [ Google Scholar]
- Norris J. Expert Pain Management. Philadelphia: Lippincott Williams & Wilkins; 1997. p. 378-9.
- Wells N, Pasero C, McCaffery M. Improving the quality of care through pain assessment and management. In: Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville, MD: Agency for Healthcare Research and Quality; 2008. p. 469-89.
- Bhakta HC, Marco CA. Pain management: association with patient satisfaction among emergency department patients. J Emerg Med 2014; 46(4):456-64. doi: 10.1016/j.jemermed.2013.04.018 [Crossref] [ Google Scholar]
- Cullison K, Carpenter CR, Milne WK. Hot off the press: use of shared decision-making for management of acute musculoskeletal pain in older adults discharged from the emergency department. Acad Emerg Med 2016; 23(8):956-8. doi: 10.1111/acem.12985 [Crossref] [ Google Scholar]